

Abstract
Aim
Elevated D-dimer post-anticoagulation cessation is a recognised risk factor for recurrent venous thromboembolic events (VTE). In particular, raised D-dimer post cessation has been associated with increased risk of recurrence in unprovoked major VTE. Currently in Australia, D-dimer has not been widely used in practice to stratify the risk of VTE recurrence. This study aims to retrospectively analyse the effect of routine D-dimer testing and it's association with VTE recurrence.
Methods
A retrospective evaluation was performed on 1024 patients with a diagnosis of VTE at a tertiary hospital in Australia between January 2013 and December 2016. Data collected included demographics, results and timing of D-dimer testing and serial imaging results.
Results
1024 patients were reviewed with a total median follow up of 12 months (range 0-59 months). D-dimer was tested in 189 patients (18.5%) within 90 days after cessation of anticoagulation. Of these patients, median age was 58 (18-92) and 55.3% (n=105) were female. 33.3% (n=63) had isolated distal deep vein thrombosis (IDDVT), 66.3% (n=126) had above knee DVT (AKDVT)/pulmonary embolus (PE), 54.5% (n=103) of VTE were provoked.
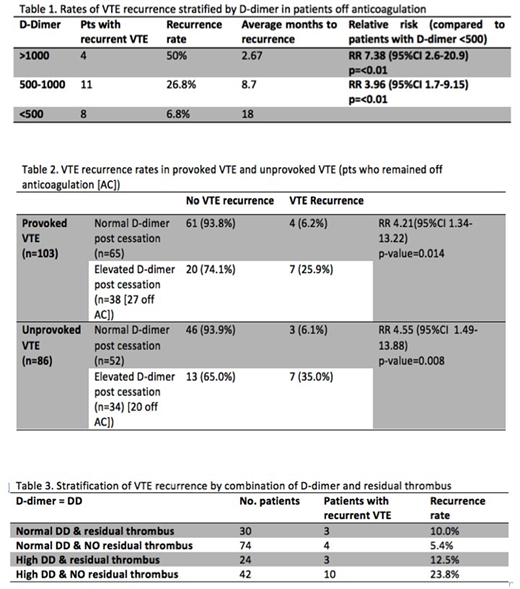
Abnormal post cessation D-dimer (>500) was found in 72 patients (37.9%). Of these, 25 patients were restarted on anticoagulation; one had recurrent VTE whilst on low dose apixaban 2.5mg BD and one had recurrence after cessation of anticoagulation at a later date. Patients with elevated D-dimer post cessation had a higher rate of recurrence with the highest risk in patients with D-dimer >1000 (RR 7.38, p=<0.01) outlined in Table 1.
Of the 164 patients with post cessation D-dimer testing who remained off anticoagulation there were a total of 24 (12.6%) episodes of recurrent VTE. Elevated D-dimer post anticoagulation cessation was a significant risk factor for recurrence in both provoked VTE (RR 4.21, p=0.01) and unprovoked VTE cohorts (RR 4.55, p=0.008) outlined in Table 2. When provoked VTE were sub-categorised, raised D-dimer demonstrated the most statistical significance in VTE provoked by travel (RR 13.5 p=0.06).
Of the patients with post anticoagulation cessation D-dimer testing 170 patients (89.9%) had repeat imaging to assess for residual thrombus. In the subgroup of patients with no residual thrombus, elevated D-dimer was a significant risk factor for VTE recurrence (RR 6.4, p=<0.01). Patients with normal D-dimer and no residual thrombus had the lowest rate of recurrence 5.4% (n=4) see Table 3.
When stratified by type of VTE, elevated D-dimer post anticoagulation cessation was significantly related to risk for recurrence in the overall IDDVT sub-cohort (RR 4.09, p=0.007). This was not significant for the AKDVT/PE sub cohort (RR 3.24, p=0.079). However, for patients with unprovoked AKDVT or PE, having D-dimer tested post anticoagulation, regardless of result, was associated with lower rates of VTE recurrence RR 0.30 (p=0.02) compared to those who had no D-dimer testing as part of follow-up.
Conclusion
Post treatment D-dimer testing may have a clinical role in stratifying the risk of VTE recurrence along with repeat imaging to detect residual thrombus. Elevated D-dimer post anticoagulation cessation is associated with increased risk of VTE recurrence for both provoked and unprovoked VTE with highest risk in patients with D-dimer >1000. Patients with no residual thrombus and a negative D-dimer post anticoagulation cessation had the lowest rate of recurrence. In the subgroup of patients with provoked VTE and IDDVT a positive D-dimer post cessation was associated with 4.21 and 4.09 relative risk of recurrence respectively, suggesting that the role of D-dimer testing can be extended to these subpopulations. Interestingly, in patients with unprovoked AKDVT or PE, having post-cessation D-dimer testing performed, regardless of result, was associated with a significantly lower rate of VTE recurrence compared to patients without D-dimer testing, which may be related to specialist review and recommencement of anticoagulation in high-risk patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal